|
Public support plummeted and opinion turned against Mary Mallon in
1915 because of her conscious return to cooking when people believed
she should have learned her lesson. "The chance was given to her
five years ago to live in freedom," editorialized the
New York Tribune, and "she deliberately elected to throw it
away." Historians have since that time been no more lenient in their
assessment of Mallon's informed return to cooking. In 1994, Robert
J. T. Joy put it directly: "Consider that Mallon disappeared for
five years, and used several aliases and went straight back to
cooking! ... Now, as far as I am concerned, this verges on assault
with the possibility of second degree murder. Mallon knows she
carries typhoid, knows she should not cook—and does so."
To be sure, Mary Mallon was not entirely blameless when she
knowingly returned to cooking in 1915, but the blame must be more
broadly shared. Much of what Mallon did can be explained by events
greater than herself and beyond her control. It is only in the full
context of her life and the actions of the health officials and the
media that we can understand the personal position of Mary Mallon
and people like her—people whom society accuses of endangering
the health of others—and can hope to formulate policies that
will address their individual needs while still permitting
governments to do what they are obligated to do, act to protect the
public's health.
 Mary's straits
Mary's straits

Mallon was not a free agent in 1914, when she returned to cooking.
Consider her circumstances. She had been abruptly, even violently,
wrenched from her life, a life in which she found various
satisfactions and from which she earned a decent living. She was
physically separated from all that was familiar to her and isolated
on an island. She was labeled a monster and a freak. [For more on
the quarantine of Mary Mallon, aka "Typhoid Mary," see
In Her Own Words.]
She was not permitted to work at a job that had sustained her, but
she was not retrained for any comparable work. If Ernst J. Lederle,
the New York City Health Commissioner who had released her in 1910,
helped her find a job in a laundry, it did not provide the wages or
job satisfaction to which she had previously become accustomed. Nor
did it provide the social amenities, as limited as they were, of
domestic work in the homes of New York's upper class. The health
department, for all of Lederle's words of obligation to help her in
1910, did not provide her with long-term gainful employment.
Neither did health officials, who precipitously locked Mallon up,
succeed in convincing Mallon that her danger to the health of people
for whom she cooked was real and lifelong. The medical arguments
that carried weight among the elite at the time and have become more
broadly convincing since did not resonate with her. There was no
welfare system to support her. There was no viable "safety net,"
practical or intellectual, for an unemployed middle-aged Irish
immigrant single woman.
Hard choices
So she did what many other healthy carriers since have done:
returned to work to support herself. And the health department
responded by doing what it felt it had to do when faced with a now
very public uncooperative typhoid carrier: returned her to
isolation. New York health officials did not isolate all the
recalcitrant carriers it identified; many who had disobeyed health
department guidelines were out in the streets during the years
Mallon remained on North Brother Island, the East River islet where
she was quarantined. But officials had reason to act as they did.
And so did Mary Mallon.

Health officials chose not to deal with their first identified
healthy carrier in a flexible way.

In other words, there were choices for both the health officials and
Mary Mallon, and judgment, when we make it, should take this full
context into account. Events could have evolved in a different
pattern. If tempers had not been raised to fever pitch in 1907, when
Mallon was first quarantined on North Brother Island, and
positions not solidified, various compromises and possibilities
would have been available for education, training, and employment, all of which might have led to decreasing the
potential of Mallon's typhoid transmission.
Health officials, who certainly held the reins of power most
tightly, chose not to deal with their first identified healthy
carrier in a flexible way. They chose to make an object lesson of
her case. But it was a choice. If they had shown some personal
respect for how difficult it was for Mary Mallon to cope with what
happened to her, it is conceivable that she would have responded in
kind and come to respect their position. As it happened, neither
side considered the other, and communication was stopped short.
Proper treatment
How can we address the problem that is now, still, again,
before us? Shall we insist on locking up the people who are sick or
who are at risk of becoming sick because they threaten the health of
those around them? Our own situation in large part determines how we
think about these questions and informs our various responses to
this public health dilemma. We can view people who carry disease as
if they consciously bring sickness and death to others—like
the demon breaking skulls into the skillet, as a 1909 newspaper
illustration depicted Mary Mallon [see image at right above]. We can
view such people as inadvertent carriers of disease, as innocent
victims of something uncontrollable in their own bodies. We can see
disease carriers as instruments of others' evil, as victims of
society's or science's perversity.
Wherever we position ourselves, as individuals and as a society, we
must come to terms with the fundamental issue that whether we think
of them as guilty or innocent, people who seem healthy can indeed
carry disease and under some conditions may menace the health of
those around them. We can blame, fear, reject, sympathize, and
understand: withal, we must decide what to do. Optimally, we search
for responses that are humane to the sufferers and at the same time
protect those who are still healthy.
The conflict between competing priorities of civil liberties and
public health will not disappear, but we can work toward developing
public health guidelines that recognize and respect the situation
and point of view of individual sufferers. People who can endanger
the health of others would be more likely to cooperate with
officials trying to stem the spread of disease if their economic
security were maintained and if they could be convinced that health
policies would treat them fairly. Equitable policies applied with
the knowledge of history should produce very few captives to the
public's health.


|

|
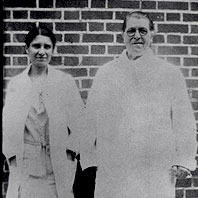
Mary Mallon (wearing glasses) photographed with
bacteriologist Emma Sherman on North Brother Island in
1931 or 1932, over 15 years after she had been
quarantined there permanently.

|
|
|
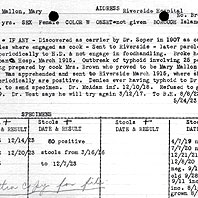
An old file card detailing results from tests on stool
specimens from Mary Mallon gives a capsule history of
her capture and quarantine.
|
|

|
Part of the New York American article of June 20,
1909, which first identified Mary Mallon as "Typhoid
Mary."
|
|
|
