
When he was struck down by a heart attack in January 2008, at the age of 74, Judah Folkman was still brimming with ideas for research—work his colleagues continue to pursue. 
In the early 1960s, while working in a Navy lab with a fellow young doctor named Fred Becker (right), Folkman made an observation that would shape the rest of his career. 
Folkman continued to investigate the puzzling phenomenon of new blood vessel growth, which he called angiogenesis, at Children's Hospital Boston in the late 1960s. 
When Folkman was appointed chief of surgery at Children's at the age of 34, he was the youngest person ever to hold the position. He somehow found time to also do basic scientific research. 
Throughout the 1970s and early 1980s, Folkman had to withstand not-so-subtle skepticism about his theory of angiogenesis. 
With Folkman's encouragement, Donald Ingber, at the time a post-doctoral researcher, discovered one of the first known angiogenesis inhibitors—and it all started with an accident. 
Perhaps even more than an accomplished surgeon and pioneering researcher, Folkman was a beloved mentor. 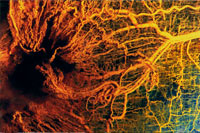
Learn more about Folkman's great epiphany, and how tumors recruit blood vessels such as these, in Angiogenesis Explained. |
Judah Folkman once said, "Science goes where you imagine it." His imagination took him—and science—in unexpected directions. In 1961, while working as a young surgeon in a U.S. Navy lab, Folkman glimpsed a hidden truth about how cancer becomes deadly. He saw that tumors without their own blood supply grew no larger than the head of a pin, and he later came to suspect that tumors actively recruit blood vessels to feed their growth. By the end of the decade, Folkman had fleshed out his theory, which he called "angiogenesis." At first scoffed at, angiogenesis is now the basis of an expansive field of medical science. It has not only led to a new class of drugs to treat cancer but also spurred new research into dozens of other diseases. In this interview, originally conducted for the 2001 NOVA program "Cancer Warrior," the father of angiogenesis talks about his early insights, the long road to acceptance of his theory, and his hopes for angiogenesis therapies. Bruce Zetter, a protégé and longtime colleague of Folkman's at Children's Hospital Boston, provided Editor's notes in July 2008. Swimming against the tideQ: What was your first "eureka" moment with angiogenesis? Judah Folkman: The first one was in the 1960s, when we saw that in isolated organs growing in our glass chambers in the Navy that the tumors implanted there all stopped at the same size. All the same size meant that something was stopping them. It took a few years to figure out it was the absence of blood vessels. I had a feeling, "This is really something important." I didn't have any idea that it would be some 30 years to try to understand the process by which tumors are able to recruit their own private blood supply and just keep going. Q: Such moments must be worth everything, especially since they're so few and far between. Folkman: Most research is failure. You go years and years and years, and then every once in a while there is a tremendous finding, and you realize for the first time in your life that you know something that hour or that day that nobody else in history has ever known, and you can understand something of how nature works. Q: When did you first lay out your theory? Folkman: A 1971 paper in the New England Journal of Medicine presented the idea in a much larger form. One, that the blood vessels in a tumor were new, and the tumor had to recruit them. Two, that it recruited the vessels by sending out some factor, which we called TAF, tumor angiogenesis factor, because we didn't know what it was. Thirdly, we put forward the idea that these [angiogenesis factors] would bring in the vessels. And fourthly, that if you could turn this process off, the tumors should stay as small as [the ones] in the thyroid gland and in the lining of the abdomen that I had seen in surgery, where they are all the same size and tiny but without blood vessels. [Bruce Zetter editor's note: We now have confirmed that, indeed, tumors can only grow into tiny, pinhead-size spheres without a blood supply. If they stay this size, they are not harmful. Consequently, if we could prevent all new tumors from attracting blood vessels, there would be fewer large tumors and fewer deaths from cancer. Also, if we could take large tumors that are already supported by many blood vessels, and make those blood vessels disappear, we should be able to shrink the tumor down to a size where it is no longer harmful. Recent research suggests that most adults have many small, pinhead-sized tumors in organs such as the breast, prostate, cervix, and thyroid but that these tumors rarely do us harm. It is only when they become angiogenic—attract new blood vessels and grow large—that they become harmful.] Q: Did you ever fear you were jumping the gun, since much of the verifying research had yet to be done? Folkman: I remember in some early grants I wrote that I outlined what I thought would be the whole future—there would be possible inhibitors and stimulators [of angiogenesis]. You never these days lay all that out in a grant; you focus it. Well, I got cold feet and thought, "Oh, I'm giving away too much." Now, Dr. John Ender's lab was right next to mine. He had won the Nobel Prize for the polio virus and was a very great scholarly gentleman. I showed him this grant and said, "I'm worried that I'm giving away too much." He read it right there. I remember him taking out his pipe, and he said "It is theft-proof. You'll be able to work at your own pace I figure for 10 years before anybody is going to believe this." He thought maybe these ideas were right, but I'd never be able to convince anybody without dozens of experiments. It turned out that hundreds of experiments were necessary over many years. Q: Was it a particularly long road because you were a surgeon and not a full-time researcher? Folkman: Surgery has the disadvantage that the training takes so long and is so physically demanding. It's like training for the Olympics practically. There's often little time for any kind of research or scholarly work, and surgeons often do not have any ability to have the very long period of scientific training that basic scientists have. So surgeons often are ridiculed because they are thought not to be able to do research. Yet many great, interesting, and important advances have come from surgeons. Q: Which is harder in your experience, being a doctor or being a researcher? Folkman: Clinical medicine has tremendous feedback, so the people who work in it are willing to work night and day. Patients call you up all the time and say, "You saved my son's life," and all that. Research is the opposite. It's just years of frustration. You have to live with experiments that don't work and grants that don't get funded. You have nothing to show for it. You've got critics all over, and scientists are sometimes mean to each other; they criticize the ideas in the name of scientific skepticism. It's not an easy life. You know that line, "I've been rich, and I've been poor, and rich is better"? Well, it's easier to be a physician than to be a researcher. I've been both, and physician is easier. Q: What gave you the confidence to go on? Folkman: Well, I always thought of it in an amused way, because I knew something that no one else knew, and I had been at the operating table. It wasn't the surgeons who were criticizing; it was basic scientists. And I knew that many of them had never seen cancer except in a dish. I knew that they had not experienced what I had experienced. The idea of tumors growing in three dimensions and needing blood vessels in the eye, in the peritoneal cavity, in the thyroid, and many other places, and the whole concept of in situ cancers and tumors waiting dormant—I had seen all that. So I kept saying, "The ideas, I think, are right, and it will just take a long time for people to see them." The tide turnsQ: So when did perception of your work start to change among researchers? Folkman: By about the end of the 1970s people began to say, "Okay, there are new vessels, we agree. But it's a side effect of dying tumor cells. It's like pus in a wound." When Robert Auerbach came [to our lab] as a sabbatical professor, that was the conventional thinking. But he did the experiment that disproved that, [and published it in] a single, crystal-clear paper. He put live tumor cells in one eye of a rabbit, and he put dying tumor cells in the other, and no blood vessels came to those [dying cells], only to the live ones. He said they must be live in order to recruit the private blood supply. That single paper changed a lot of people's thinking. I would say the watershed year for complete change of thinking amongst scientists was about 1989. By then there were such strong experiments coming from our lab, from Genentec's lab, and from Europe that tumors not only induced new vessels but were angiogenesis-dependent, that most scientists began to accept that. But it took a long time. Q: In 1984, your team published a paper in Science about the discovery of the first angiogenic factor the year before. That must have stirred things up. Folkman: That paper had great transforming power. Almost overnight many, many, many critics were transformed into competitors, because people began to see that there was a molecule in this field. That was the first; there are now 17. I was beginning to wonder whether there would ever be an angiogenic factor. We had spent so many years on it. In general, if you don't find something in four or five years, people say it's not there. In research, there's a very fine line between persistence and obstinacy. You do not know whether if you're persistent a little while longer you'll make it, or whether you're just being obstinate [and it] doesn't exist. And, of course, you can keep on going, stay with an idea too long—[that's] called pigheadedness. I was beginning to think we had crossed that line and were spending money and had nothing to show for it. When that came [the discovery of the first angiogenic factor produced by a tumor], that was a great sense of relief, that it actually did exist. It's like Sputnik. The U.S. had all the information to put up a satellite, but we didn't until Russia did. Then suddenly we said, "Oh, you can do it." Once people saw that it was possible [to find angiogenic factors], they began to look and found other ones. [Bruce Zetter editor's note: An angiogenic factor is anything that can stimulate the growth of new blood vessels. When he first had the idea that tumors were dependent on blood vessels for their growth, Folkman thought that there would be just one such factor, and he named it "tumor angiogenic factor," or TAF, without knowing exactly what it was. Critics asked him to identify the nature of TAF, and in 1984, he and Michael Klagsbrun and Yuen Shing showed the chemical makeup of the first tumor-derived angiogenesis factor. Today, we know that there are more than 20 angiogenesis factors, including VEGF (vascular endothelial growth factor) and FGF (fibroblast growth factor). As tumors grow in the body, they often make more and more different kinds of angiogenesis factors over time. This suggests that drugs that block just one particular angiogenesis factor may work best on tumors that produce predominantly that one factor.] An accidental discoveryQ: It took just as long to find angiogenesis inhibitors, those that inhibit blood-vessel growth, right? Folkman: Yes. In 1980 came interferon, in 1981 or 1982 came platelet factor 4. These were the first two. By then we said there are angiogenesis inhibitors. Q: And a member of your team found the third one by accident? Folkman: Yes. Don Ingber was an M.D., Ph.D. who had come up from Yale and was studying endothelial cells [cells that line the interior of blood vessels]. Every time a new building was being built outside Children's Hospital, funguses would come into the windows, and you'd get contamination of these in the cell cultures. When you got a fungus growing in there, it would turn turbid, and the little dish of cells would all die and float. So Don had a set of endothelial cells, and there was a fungus contaminant at one end of the dish. He called me and said you have to come in and see this, because there's something different. The cells were not dying—they were just backing away. He said there's something coming from the fungus that is stopping the endothelial cells. Now, what's important is that anyone else in the lab would have thrown that out. There were signs all over the lab that said if your cell culture becomes contaminated with a fungus, you must throw it out, because it will infect the whole lab. I used to get upset with people who didn't. So Ingber called and said, "I would like permission to keep this culture." That led to the isolation of a compound [called TNP-470] that is today in clinical trial. In animal tumors it has a very broad spectrum antitumor effect. It was a little stronger than platelet factor 4 and much stronger than interferon. So that was a purely serendipitous discovery. [Bruce Zetter editor's note: When new drugs are tested, the first set of trials (Phase 1) is undertaken to see if the drug has any toxicity or side effects. When TNP-470 was tested, doctors were encouraged to see some positive responses in some of the patients, but there was some toxicity that prevented the drug from being used in more trials. This included neurological effects such as increased anxiety, trouble concentrating, and trouble walking. At the time of his death, Folkman was actively working on new forms of TNP-470 that would reduce toxicity yet work just as well against tumors. His colleagues are continuing this work.] Testing drugs, treating patientsQ: Two angiogensis inhibitors your team discovered—endostatin and angiostatin—are now in clinical trials. How do you feel about the patients who are trying your new therapy? Folkman: Patients going through these trials are in a desperate situation. Nothing else has worked, there's little time left—and they have a fast clock running. We all have a clock but theirs is very fast. And so they're very scared. Therefore, from a physician's point of view, you have to go out of your way to make sure that not only they understand [the uncertainties] but that you don't destroy their hope. Q: A friend of mine keeps asking me, since these people in clinical trials are terminally ill, why don't you give them a lot of, say, endostatin? Folkman: What if a lot turns out to be dangerous? Then you've made their life worse than it was. The ethic is "above all do no harm." To build on that rule, an old rule in medicine, the Food and Drug Administration through federal laws has said that when you start testing a new drug, you must start much lower than you expect it to be effective. That is the safe thing to do. But it creates an ethical problem that that might be an ineffective dose. Q: And even with larger doses, you don't want to raise anyone's hopes too high. Folkman: Yes. Many times when you see the very first experiments in mice and then you try it in people, there's always a great deal of hope among patients and physicians. It's the same problem we have with endostatin and angiostatin. But there's also a high risk of let-downs or raising expectations too high. Because when you go from the laboratory to people, there's a high failure rate. All mice are like identical twins; all people are not. Our view is that, in time, angiogenesis inhibitors will be added to chemotherapy, added to radiotherapy, added to immunotherapy, added to gene therapy, and added to one another. And eventually, one by one, doctors will have a whole arsenal of these, and that may improve things. We hope. Q: What are your greatest hopes? Folkman: There are many. Even if endostatin or angiostatin should fail [in clinical trial], the principles are solid, they've been established over 30 years. They've been replicated by laboratories around the world. Demonstrating proof of principle in the clinic that you can control tumors or slow them down or regress them by anti-angiogenic therapy is the hope—that's what we're working on. Eventually we hope that will come, even if it means that you have to give two angiogenesis inhibitors together, because that's what we have to do in mice to get a really good tumor eradication. So physicians in the next decade may have an arsenal of angiogenesis inhibitors, possibly 10 or 20, and they can combine them and choose among them and add them to other therapies to increase the power of the control that doctors have over cancer. [Bruce Zetter editor's note: Although some patients seemed to improve while on endostatin, the results in the United States were not sufficiently positive to justify continuing with development of the drug in this country. More recently, scientists in China have made a modified form of endostatin (Endostar), and they have reported some success with that form of the drug. Additional work will be needed to determine if this drug is effective and worth bringing back into trials in the U.S. Before his death, Judah Folkman was very gratified to see
that other anti-angiogenic drugs had been developed that were clearly active
against certain cancers. These include Avastin, an FDA-approved drug that
blocks the effect of VEGF, a tumor-derived angiogenesis stimulator. In
addition, several drugs already in use treating cancer patients have now been
shown to have anti-angiogenic activity in addition to other modes of action.
This list includes, among many others, Velcade, Thalidomide, Tarceva, and
Sutent.]
|
"I had a feeling, ‘This is really something important.' I didn't have any idea that it would be some 30 years to try to understand the process." "Most research is failure. You go years and years and years, and then every once in a while there is a tremendous finding." "Surgeons often are ridiculed because they are thought not to be able to do research." "Almost overnight many, many, many critics were transformed into competitors." "Physicians in the next decade may have an arsenal of angiogenesis inhibitors." |
|||||||||
|
Interview originally conducted by producer Nancy Linde for the 2001 NOVA program "Cancer Warrior," and edited by Susan K. Lewis, editor of NOVA online |
|||||||||||
|
© | Created July 2008 |
|||||||||||