The Journey Begins | Dear Film Crew: Help! | On Call | Alex's Case
September 20, 1996
The "Medical Tower" apartments next to New York Hospital
Room 1019
At 6:00 a.m. this morning, Tom (the principal cinematographer), and Peter
(the principal sound person) returned to their post at Jamaica Hospital.
Jeffrey (the second camera person) and I returned to our post at New York
Hospital. We each went about the business of setting up equipment;
 re-introducing ourselves to the paramedics, emergency dispatchers, trauma
teams; and directing the production assistant to secure for us the
necessary production supplies and food for our locations.
re-introducing ourselves to the paramedics, emergency dispatchers, trauma
teams; and directing the production assistant to secure for us the
necessary production supplies and food for our locations.
That evening, at 5:53, my beeper went off. Since it was our first day back
on call, I assumed that the emergency dispatcher at New York Hospital was
testing our system. But the beeper read 111, which was the signal for Team
A at Jamaica to race to the emergency room. Just as during our first
period on call, the drill was for the team to go ahead and film 1 or 2
camera rolls, no questions asked. Then they would punch one number on
their specially programmed cell phone to consult with me. I made sure my
cell phone battery was charged and waited for the call.
Some time later, a call came, but it wasn't from Team A. It was from Dr.
Ghajar. There was a severe head trauma case in the emergency room at
Jamaica. It was a young boy, who had been struck by a car while crossing
the street. He was in a coma.
I alerted Jeffrey to prepare to film Dr. Ghajar driving to Jamaica. It was
about 6:30 p.m. Shortly thereafter, the crew at Jamaica finally called
from the emergency room. Usually, Peter would phone me, while Tom would
continue to watch a given case, just to be sure it wasn't a false start.
This time, Tom was on the phone, and his voice was shaking. The case was
serious. This was no false start. He and Peter had been following the
basic resuscitation by the trauma team—the ABC's, for airway, breathing
and circulation—and were preparing to follow the patient up to the CT
scan.
Jeffrey and I meet Dr. Ghajar at his car. We start rolling when Dr. Ghajar
calls Jamaica on his car phone. Part of the conversation is in the final
program:
Dr. Jam Ghajar: Hello, Venu.
Dr. Venu: Yeah?
Dr. Jam Ghajar: Yeah. Did you examine him?
Dr. Venu: Yeah.
Dr. Jam Ghajar: Does he, does he open his eyes?
Dr. Venu: No, he's not.
Dr. Jam Ghajar: He's not opening his eyes.
Dr. Venu: No.
Dr. Jam Ghajar: Okay, can you have the ventric set and a cut-down set?
When colleagues watch the film, they assume that we later simulated the car
drive and phone call to Jamaica. But it's real.
And so is, of course, what unfolded in the emergency room.
None of the false starts prepared us for what we saw that night. The young
boy was clearly in trouble. His body was struggling to breathe—in a very
shallow but tortured way—so he was immediately hooked up to a respirator.
The trauma team had to keep suctioning blood that repeatedly accumulated
in his mouth. All sorts of lines—wires for monitors, tubes for IVs—went
into his lifeless body. I just remember standing there with the crew,
thinking, 'Oh, my god, this is really happening.'
Even when the popular and well-produced medical drama series get it
"right," the real thing is very different. In television dramas, physical
movements are rehearsed; in a real-life emergency room, no one has
choreographed the action. There are no actors, no scripts. Real trauma
team members don't wait for someone else's line to end before they start
talking; everyone is talking at the same time, asking concerned questions,
 barking tense orders—cursing if something isn't working. Watching actors
try to convey tension, fear, and concern is a whole lot different than
seeing real people feel these very real emotions, as a child lays
critically injured, near death.
barking tense orders—cursing if something isn't working. Watching actors
try to convey tension, fear, and concern is a whole lot different than
seeing real people feel these very real emotions, as a child lays
critically injured, near death.
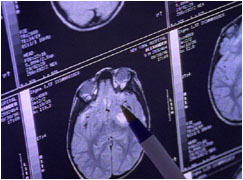
Ghajar gets into his scrubs upon arrival and reviews the CT scans. There
are definitely signs of brain swelling. The brain could strangulate
without more room, and one way to make space is to drain clear fluid that
the body makes and replenishes on its own, filling cavities in the brain
called ventricles. Ghajar drills a hole through the patient's skull and
inserts a catheter. The trauma team gathers to watch the procedure. When
the catheter hits the brain cavities, clear fluid immediately drains out,
showing the pressure already building in the patient's skull.
His name is Alex, he's nine years old, and he was excitedly racing home
from karate class that evening, to tell his mother that he had just gotten
his second yellow belt, when he was struck by a car.
At the moment his family sits in a private conference room at Jamaica
Hospital, down the hall from the trauma room where all the activity has
been unfolding. Now, at what could very well be the lowest point of their
lives, I must ask them for permission to follow the case.
When I enter the private conference room, I close the door behind me. I
hear the spunky voice of a little girl, peaking out from behind her mother:
"Don't close the door on your finger," she cautions. This is Alex's
three-year-old sister, Arianna. And for a brief moment, she breaks through
the grief in the room, causing everyone to smile or laugh nervously. I
start to introduce myself and the project, but I hear my voice shaking and
cracking, as if I am listening to someone else. It is at this moment that
I look directly at Alex's mother, and see a most amazing, welcoming, and
warm look in her eyes. "I know what you want to do," she says.
Friday, September 20, 1996, near midnight
In a transfer ambulance, on FDR, driving south towards New York Hospital
Jamaica Hospital does not have a pediatric intensive care unit, so Alex
must be transferred to one at New York Hospital. The paramedics who come
 to pick him up know Jeffrey and me from the many hours we've spent at our
post, so they offer to let us come along in the ambulance.
to pick him up know Jeffrey and me from the many hours we've spent at our
post, so they offer to let us come along in the ambulance.
From this point on, every time that Alex must be moved, it will be a
labor-intensive ordeal. Because Alex must be unhooked from the respirator,
a doctor must sit by his side in the ambulance and push air into his lungs
with an ambu-bag. A paramedic immobilizes Alex's head with rolled towels
on either side—and he too sits by Alex for the entire ride, simply holding
the patient's head in place, trying to absorb the shock from New York
city's potholes. In an age of high-tech medicine, this whole scene is at
once poignant and alarming.
Ghajar arrives at New York Hospital as the pediatric team settles Alex into
an ICU bed and hooks him up again to a respirator and various monitors.
The main task over the next several days is to help keep a constant vigil
on the pressure inside Alex's head. It's called ICP, for intracranial
pressure, and it's hovering around 20 mm of mercury. Ten is average for a
healthy person, so the medical team continues to drain fluid from Alex's
brain.
I've read that "death" is the one word you'll never hear from a doctor, but
Ghajar is different. In a conference at New York Hospital to update Alex's
mother, around 1 in the morning, he says, "The question is, 'What'll he be
like ultimately?' Right now, we don't address those kind of questions.
Right now, it's kind of life and death. We're trying to prevent the brain
from swelling further. That's why he's here in the intensive care unit."
Saturday, September 21, 1996, 11 a.m.
Alex's ICU room, New York Hospital
"Sorry, Alex, we'll be done in a second, big guy. I'm just going to take a
picture of your head." Jean Marie
Cannon, a nurse in the pediatric intensive care, is carefully helping to
position Alex for his second CT scan. Watching her gently explain what's
 happening to a patient in a deep coma is reassuring. For a second, I
forget the dire circumstances.
happening to a patient in a deep coma is reassuring. For a second, I
forget the dire circumstances.
Ms. Cannon's bedside manner is also comforting to Alex's parents. She's
sees this as a critical part of her job. "In Alex's case, you've got a
child who one minute is running around and is healthy and happy and the
next minute is laying in a hospital bed, critically ill. And the parents
have no chance to, to adjust to that. They're usually in shock, and coming
into the ICU such as this, they're just overwhelmed by the technology and
the buzzers and the monitors—and all of the things that we're doing to
keep their son alive and to keep him healthy."
Cannon and the rest of the intensive care team must perform a number of
tasks to keep other parts of a head-injured patient's body from
deteriorating. For example, "We take blinking for granted, but comatose
patients often don't close their eyes all the way. We need to keep the
eyes lubricated, or they can get corneal abrasions or little scratches on
his cornea."
Also, for patients who have been intubated—that is, who have a breathing
tube inserted into their trachea—the team must take over the bodily
function of swallowing by periodically suctioning the patient's mouth.
"With that tube in, a patient can't swallow, and therefore they will pool
mucous and secretions in their mouth, and we'll need to clean."
The feet of a coma patient are put into cuffs to prevent the patient's
Achilles tendon from shortening, a condition called "foot drop," that can
severely hamper learning how to walk again.
But the most important job for the entire team in the first week after
injury is to constantly monitor the pressure inside the patient's skull.
And on this day, beginning about 48 hours after the injury, Alex's pressure climbs into the
30s, well above a safe level. The average for a healthy person is 10;
around 20 would be acceptable in a head-injured patient. 30 is worrisome
and requires intervention if draining alone cannot bring it under control.
Because swelling can choke off the supply of oxygen-carrying blood, Alex's
team raises his blood pressure, to force more blood into his brain, during
this period of high ICP.
Ghajar also counsels the parents not to stimulate Alex, advising them to
try not to talk to him. Earlier in the day, when a lot off family members
were visiting and talking around Alex's bed, his ICP rose, and he became
agitated. There's a misconception, Ghajar believes, on the part of the
public, that the earlier you can stimulate a coma patient to "wake up," the
better off the outcome. But in fact, during this critical period right
 after the accident, it is important to keep the intracranial pressure down,
in order to maintain a steady flow of oxygen to the brain. That's what
will improve outcome. And sometimes that means not talking to the patient
for a period of days.
after the accident, it is important to keep the intracranial pressure down,
in order to maintain a steady flow of oxygen to the brain. That's what
will improve outcome. And sometimes that means not talking to the patient
for a period of days.
While there are physical signs, such as a rise in ICP, that the comatose
patient may be aware of the presence of family members, patients do not
remember the experience when they emerge from the coma. The brain is too
injured to lay down memories, Ghajar explains.
It occurs to me that this is related to why head-injured patients suffer
retro-amnesia; the parts of the brain needed to convert a short-term memory
to a long-term memory are shut down. This is probably why I can't remember
the days leading up to my childhood concussion.
Alex's mother did not sleep last night. Her expressive face shows grief
and fear. I now understand why my own parents rushed me to the hospital
when I fell off the swing. Even though I did not lose consciousness, I
suddenly ceased recognizing familiar people. I had lost my association
with the past, and therefore part of my sense of self.
Now, Alex's parents stand watch, waiting for their son to emerge.
"The hardest part of dealing with patients [in coma] is that we don't have
any answers for these parents," Cannon says. "We can't say, 100 percent,
'Your son is going to be fine, or your son is not going to be fine.' The
hardest part is the uncertainty—and not knowing what the outcome is going
to be six months down the road."
Wednesday, September 25, 1996, 9:30 a.m.
Alex's ICU room, New York Hospital
When a patient is in a coma, there are few things the doctor can do to
examine him. One common approach is to pinch the patient just below the
 collarbone, to see how the patient responds. Two days ago, when Ghajar
pinched Alex, he reached toward the noxious stimuli with his hand, a good
sign that he was establishing a new level of consciousness.
collarbone, to see how the patient responds. Two days ago, when Ghajar
pinched Alex, he reached toward the noxious stimuli with his hand, a good
sign that he was establishing a new level of consciousness.
Today, Ghajar walks into Alex's ICU room and pinches him again. This time,
Alex opens his eyes for the first time! Alex cannot yet interact with his
environment. He does not recognize family members. He has no idea what's
going on. But eye-opening means that Alex's brain is re-establishing
cycles of sleeping and waking. Technically, he's no longer in a coma, and
Ghajar is no longer concerned about the pressure inside his brain.
I had gathered the crew to film today. Alex's eyes had been fluttering
yesterday, and we all hoped he might just open them. When he did, I
gasped. It was as magic a moment as I suspect I'll ever experience.
Most coma patients open their eyes within a week, so Alex, thus far, is on
an expected course. We can't wait for him to emerge more fully. And we
assume, because his pressure is down and his eyes are opening and closing
that it's a straight shot to recovery now.
Little do we know that the emotional roller coaster is about to enter and
long and tortuous dip.
Wednesday, October 2, 1996
Alex's ICU room, New York Hospital
Vegetative state. These are two words that you never want to hear in
connection to a loved one, Alex's mother says. But her son is in one.
Since Day Five when he first opened his eyes, he has not shown any
conscious behavior. He does not respond to any simple commands, such as,
"Raise your right thumb." He can't track moving objects. He is not aware
of his environment.
Regardless of how good the care after a head injury, about 10 to 20 percent of
all patients remain in a vegetative state forever. This is perhaps because
 the initial brain injury was too extensive, or the patient suffered a
period of time without oxygen after the accident.
the initial brain injury was too extensive, or the patient suffered a
period of time without oxygen after the accident.
Indeed, Alex's brain injuries from the accident are more extensive than
originally realized. He's off the respirator now, so it's easier to get an
MRI, a more detailed image than a CT scan. Ghajar and a radiology
technician review the scan.
"This MRI shows much more extensive abnormalities than the CT scan showed,"
the technician says, "including bifrontal areas of hemorrhagic contusion
and several deep white matter shear injuries in the left posterior frontal
lobe, as well as in the right frontal temporal lobe—as well as additional
area of shear injury in the high left posterior frontal lobe. There's a
large area of shear injury, which is a common sight of shear injury, in the
splenium of the corpus callosum.
"The hemorraghic contusions in the inferior frontal and temporal
lobes—that's a common location of hemorraghic contusions, because you have
a dense bone separating those two lobes, and as the brain is moving
forward, for instance, in a motor vehicle accident, the brain sort of slaps
against the bone—the bone doesn't move—and therefore the brain sort of
has to come to an abrupt stop at the bone," the technician explains.
"We also call this gliding injury, Ghajar says. "You see here, here is the
base of the frontal fossa, the frontal lobe sits on, and you can see if the
head moves forward, the brain moves in a different speed and glides across
the surface here, and this surface here is not smooth. It's very—it has
ridges in it. And what happens is the brain hits those ridges and it causes
little bleeding, little tears, and all that. To what extent they heal and
 what his eventual outcome is going to be, really you have to wait and see.
But he has significant injuries. This is not, you know, minor injuries."
what his eventual outcome is going to be, really you have to wait and see.
But he has significant injuries. This is not, you know, minor injuries."
We will continue to follow Alex's case, filming about once a month. But
this is our last day "on call." We all had hoped that Alex would respond.
We end the filming day by packing and preparing to leave our posts.
Usually, wrapping a location is an occasion for celebration, but everyone
is quiet and depressed.
Among the crew members, there is a vast range of spiritual and religious
beliefs. So I expect that everyone will have a unique way of dealing with
what tragically seems to be unfolding.
But I would later find out that after we disbanded and went to our
respective homes that night, every single team member, without exception,
said a prayer for Alex.